Free New Hampshire 2620 PDF Form
Free New Hampshire 2620 PDF Form
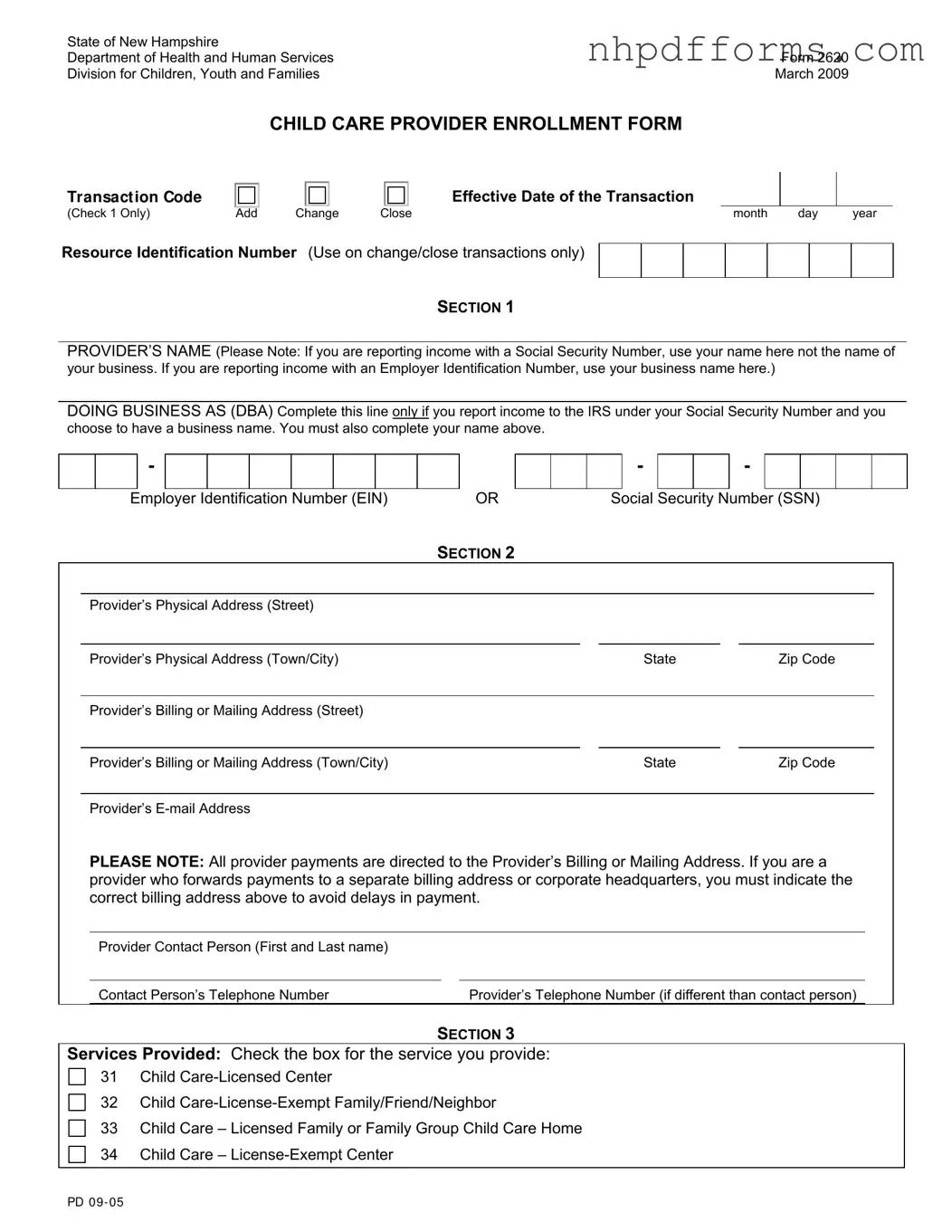
The New Hampshire 2620 form serves as a crucial document for child care providers seeking enrollment with the Department of Health and Human Services (DHHS). This form is designed to facilitate the enrollment process, ensuring that providers can receive payments for their services. It requires detailed information, including the provider's name, business name if applicable, and contact information. Additionally, providers must specify their physical and mailing addresses, as accurate information is vital for payment processing. The form also includes sections for identifying the services offered, ranging from licensed centers to license-exempt care. Importantly, the 2620 form mandates that providers report any changes, such as address updates or name changes, to maintain compliance with DHHS regulations. By completing this form accurately, child care providers can avoid payment delays and ensure they are properly enrolled in the system, thus allowing them to focus on delivering quality care to children in their communities.
State of New Hampshire |
|
Department of Health and Human Services |
Form 2620 |
Division for Children, Youth and Families |
March 2009 |
CHILD CARE PROVIDER ENROLLMENT FORM
TRANSACT ION CODE
Effective Date of the Transaction
(Check 1 Only) |
Add |
Change |
Close |
month |
day |
year |
Resource Identification Number (Use on change/close transactions only)
SECTION 1
PROVIDER’S NAME (Please Note: If you are reporting income with a Social Security Number, use your name here not the name of your business. If you are reporting income with an Employer Identification Number, use your business name here.)
DOING BUSINESS AS (DBA) Complete this line only if you report income to the IRS under your Social Security Number and you choose to have a business name. You must also complete your name above.
-
Employer Identification Number (EIN) |
OR |
- |
|
|
- |
|
|
|
|
Social Security Number (SSN)
SECTION 2
Provider’s Physical Address (Street) |
|
|
|
|
|
|
|
|
|
Provider’s Physical Address (Town/City) |
|
State |
|
Zip Code |
|
|
|
|
|
Provider’s Billing or Mailing Address (Street) |
|
|
|
|
|
|
|
|
|
Provider’s Billing or Mailing Address (Town/City) |
|
State |
|
Zip Code |
|
|
|
|
|
Provider’s |
|
|
|
|
PLEASE NOTE: All provider payments are directed to the Provider’s Billing or Mailing Address. If you are a provider who forwards payments to a separate billing address or corporate headquarters, you must indicate the correct billing address above to avoid delays in payment.
Provider Contact Person (First and Last name)
Contact Person’s Telephone Number |
Provider’s Telephone Number (if different than contact person) |
SECTION 3
Services Provided: Check the box for the service you provide:
31 Child
32 Child
33 Child Care – Licensed Family or Family Group Child Care Home 34 Child Care –
PD 09 - 05
INSTRUCTIONS FOR COMPLETION OF PROVIDER ENROLLMENT FORM
All providers of child care services who wish to receive payment from the Department of Health and Human Services (DHHS) must be enrolled and are subject to all Department rules, regulations, policies, and procedures. This is done with completion of a child care enrollment packet. No payments will be made to any provider until the enrollment process has been completed. DHHS does not withhold tax money for individuals receiving payments for services. Payment of taxes is the responsibility of the individual.
Enrollment and Billing: At time of enrollment, all providers will be assigned a Resource Identification (ID) Number. A Provider Enrollment Notice will be sent informing you that the enrollment process has been completed.
Please retain this notice! The Provider Notice will give you the information required to be entered on all billing invoices that you submit to DHHS. To be reimbursed for child care services, you must bill on
DHHS billing invoice Form 2500.
Reporting Changes: Providers are required to report all changes to DHHS such as changes of address, incorporation, or provider name. Changes must be reported to DHHS by submitting them on a new FORM 2620 and ALTERNATE
Form Completion
Transaction Code Add- Check when you request a new enrollment. Transaction Code Change- Check when you report a change, or are
Resource ID Number- Enter your Resource ID number when you report a change or request an enrollment closing. Enter your number from left to right leaving unused spaces blank at the end.
Effective Date- Enter month, day, year. This date will be your first date of enrollment, date child care services will be provided by you, the effective date of your change, or your enrollment end date.
SECTION 1
Provider Name - This line must be completed whether you report income under your SSN# or EIN# Enter your own name here if you report income to the IRS under your Social Security Number.
Enter the name of your business here only if you report income to the IRS with an Employer Identification Number.
Doing Business As- Complete this line only if you report income to the IRS under your Social Security Number. If you have a business name, enter it. You must also indicate your first name, middle initial and last name on the line provided above.
Employer ID Number or Social Security Number- Enter the number you use to report income to the IRS (Enter only one number- either the SSN# or the EIN#).
SECTION 2
Provider Address- Enter your physical and billing or mailing address. (See note on the front of this form)
Contact Person- Enter the name, telephone number and email address of the person to contact for questions.
SECTION 3
Services Provided- Check the box for the child care service you provide.
Return this form, along with a completed ALTERNATE
Department of Health and Human Services
Data Management Unit
Box 2000
Concord, NH
PD 09 - 05
| Fact Name | Details |
|---|---|
| Form Purpose | The New Hampshire 2620 form is used for enrolling child care providers to receive payments from the Department of Health and Human Services (DHHS). |
| Governing Law | This form is governed by New Hampshire state regulations regarding child care services and provider enrollment. |
| Transaction Codes | Providers must indicate whether they are adding, changing, or closing their enrollment using specific transaction codes on the form. |
| Resource Identification Number | Upon enrollment, providers are assigned a Resource Identification Number, which is necessary for all billing processes. |
| Tax Responsibility | DHHS does not withhold taxes from payments made to providers; tax obligations fall on the individual providers. |
| Required Changes | Providers must report any changes in their information, such as address or name changes, by submitting a new 2620 form along with an Alternate W-9 form. |
| Submission Address | Completed forms should be sent to the Department of Health and Human Services, Data Management Unit, Box 2000, Concord, NH 03302-2000. |
New Hampshire Load - The form caters to various needs, including new permits, renewals, and both single and multi-state trips, making it versatile for different hauling requirements.
An Emotional Support Animal Letter is a document prescribed by a licensed mental health professional that verifies an individual's need for a pet to provide significant emotional or psychological support. This letter can be obtained through various sources, including smarttemplates.net, helping to alleviate symptoms of a disability and granting important legal protections for living and traveling with the animal.
Is W4 State or Federal - By signing the form, providers agree to bill only for actual hours a child attended, ensuring billing accuracy and compliance.