Free New Hampshire 3820 PDF Form
Free New Hampshire 3820 PDF Form
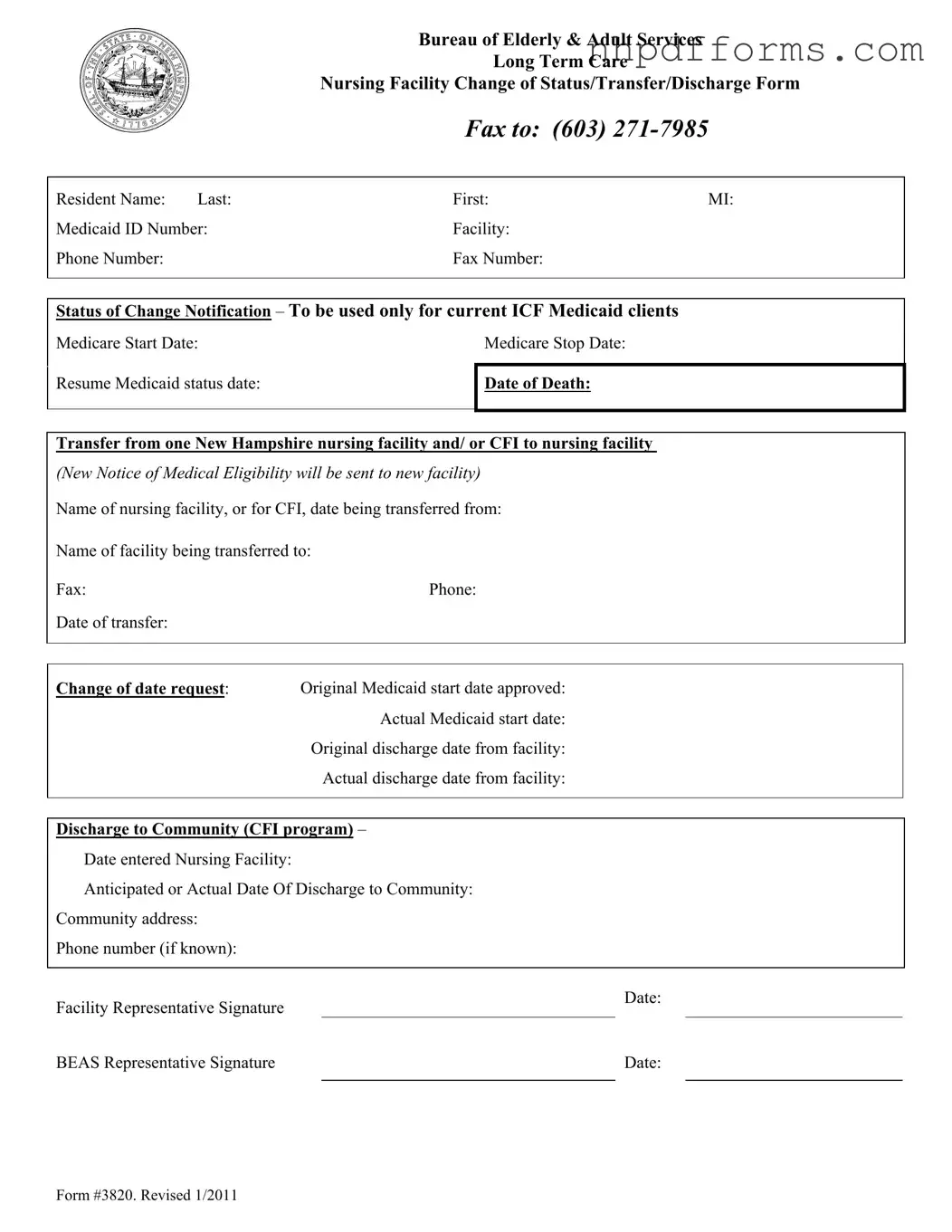
The New Hampshire 3820 form serves as a crucial tool for managing the transitions of residents within long-term care facilities, specifically in nursing homes and community-based programs. Designed by the Bureau of Elderly & Adult Services, this form facilitates the notification process for changes in status, whether it be a transfer, discharge, or other significant updates concerning a resident's care. It captures essential details such as the resident's name, Medicaid ID number, and the facilities involved in the transition. Additionally, the form records vital dates, including the start and stop dates of Medicare, as well as actual and anticipated discharge dates. For those transitioning back to community living, the form also requires information about the community address and contact details. By ensuring that all necessary information is documented and communicated effectively, the New Hampshire 3820 form plays a pivotal role in safeguarding the continuity of care for individuals in long-term care settings.
|
Bureau of Elderly & Adult Services |
||
|
|
Long Term Care |
|
|
Nursing Facility Change of Status/Transfer/Discharge Form |
||
|
FAX TO: |
(603) |
|
|
|
|
|
Resident Name: Last: |
First: |
MI: |
|
Medicaid ID Number: |
Facility: |
|
|
Phone Number: |
Fax Number: |
|
|
|
|
||
|
|
||
Status of Change Notification – To be used only for current ICF Medicaid clients |
|||
Medicare Start Date: |
|
Medicare Stop Date: |
|
|
|
|
|
Resume Medicaid status date:
Date of Death:
Transfer from one New Hampshire nursing facility and/ or CFI to nursing facility
(New Notice of Medical Eligibility will be sent to new facility) Name of nursing facility, or for CFI, date being transferred from:
Name of facility being transferred to:
Fax:Phone:
Date of transfer:
Change of date request: Original Medicaid start date approved: Actual Medicaid start date:
Original discharge date from facility:
Actual discharge date from facility:
Discharge to Community (CFI program) –
Date entered Nursing Facility:
Anticipated or Actual Date Of Discharge to Community:
Community address:
Phone number (if known):
Facility Representative Signature
Date:
BEAS Representative Signature |
|
Date: |
|
|
|
Form #3820. Revised 1/2011
| Fact Name | Details |
|---|---|
| Form Purpose | This form is used for notifying changes in status, transfers, or discharges of residents in New Hampshire nursing facilities. |
| Governing Law | The form is governed by New Hampshire state laws regarding long-term care and Medicaid services. |
| Intended Users | Current Intermediate Care Facility (ICF) Medicaid clients and their representatives must use this form. |
| Contact Information | Fax the completed form to the Bureau of Elderly & Adult Services at (603) 271-7985. |
| Revisions | This version of the form, #3820, was revised in January 2011. |
New Hampshire Load - The form outlines the necessity of daylight-only travel for permitted loads, emphasizing safety considerations during transit.
New Hampshire W4 - The form’s comprehensive design aids in the efficient processing and resolution of motions by the court.
In order to complete the process of selling a motorcycle legally in California, it is essential to use the California Motorcycle Bill of Sale form, which serves as a key legal document to prove ownership transfer. For those looking for a reliable template to facilitate this transaction, resources such as TopTemplates.info can be incredibly helpful, offering clear guidelines and necessary details about the motorcycle sale.
Is W4 State or Federal - This document outlines the operational standards and legal responsibilities for participating child care providers.